Securing AI Agents in Healthcare: Protecting Patient Data from Silent Leaks

The clinical environment is undergoing a fundamental shift: the transition from passive Large Language Models (LLMs) to Autonomous Agentic AI systems. In this new era, the line between software and staff is blurring.
Healthcare is moving beyond simple "Q&A" chatbots to Non-Human Identities (NHI)—autonomous agents that don’t just summarize text, but independently execute clinical workflows. These systems analyze Electronic Health Records (EHRs) and automate high-stakes tasks within the hospital inbox.
However, as agency increases, the surface for PHI (Protected Health Information) data leakage expands. For the healthcare CISO, the challenge is now governing the behavioral intent of agents operating without traditional human oversight.
The Rise of the "Silent Failure"
The primary risk in the agentic era is the "Silent Failure." This occurs when an agent appears to function correctly but fails hiddenly in its reasoning logic—leading to the unauthorized disclosure of patient data. According to research on Shadow AI governance, 75% of technology leaders fear these failures will lead to regulatory ruin.
Traditional Data Loss Prevention (DLP) tools are blind to LLM "reasoning paths." An AI agent may inadvertently memorize and exfiltrate sensitive identifiers—such as SSNs or medication dosages—to unmanaged third-party models. To satisfy the HIPAA Minimum Necessary Standard, security must move toward a specialized AI firewall that enforces context-aware, Attribute-Based Access Control (ABAC).
The 5 Horizons of Healthcare AI Autonomy: From Chatbots to Agents
To properly manage Non-Human Identities (NHI), hospital security teams must first understand how much "freedom" an AI has. We classify the growth of healthcare AI through five specific levels, or "Horizons." As an AI moves from answering questions to making decisions, its risk of leaking PHI (Protected Health Information) increases.
The Healthcare AI Maturity Model
Horizon 0 & 1: Basic Chatbots (Single Tasks)
Most hospitals start here. These are simple "Question & Answer" bots. They can help a patient find clinic hours or summarize a single medical document. These bots are safe because they don't talk to other systems; they only react to what you type. From a governance perspective, the main risk is someone trying to "trick" the bot into giving out administrative secrets.
Horizon 2: Deep Agents (The "Sweet Spot" for Hospitals)*
This is the current goal for the healthcare industry. Unlike a chatbot, a Deep Agent acts like an orchestrator. It can take a complex goal—like "onboard a new surgeon"—and split it into smaller tasks.
- What it does: It interacts with FHIR APIs (medical data standards) and Electronic Health Records (EHR) to summarize years of medical history in seconds.
- The Technical Edge: It decides which files to read and which tools to use to reach its goal.
Horizon 3 & 4: Role-Based Agent Teams (Full Coordination)
At this level, different AI agents talk to each other. For example, an "Admissions Agent" sends data to a "Pharmacy Agent" to automate prescriptions. Horizon 4, the Agent Mesh, is a self-managing network that fixes logistical issues, such as hospital bed shortages or medical supply chain delays, without human help.
For a hospital CISO (Chief Information Security Officer), Horizon 2 offers the best Return on Investment (ROI), but it also creates the biggest "data leakage" surface.
Because Deep Agents have the power to "summarize and synthesize," they need deep access to your most sensitive patient data. This shifts the security focus from just watching what a human types to watching what the AI agent does.
Without runtime protection a Deep Agent becomes an "Invisible Insider." It might work perfectly but could accidentally store a patient’s medical summary in an unmanaged, public cloud to save time.
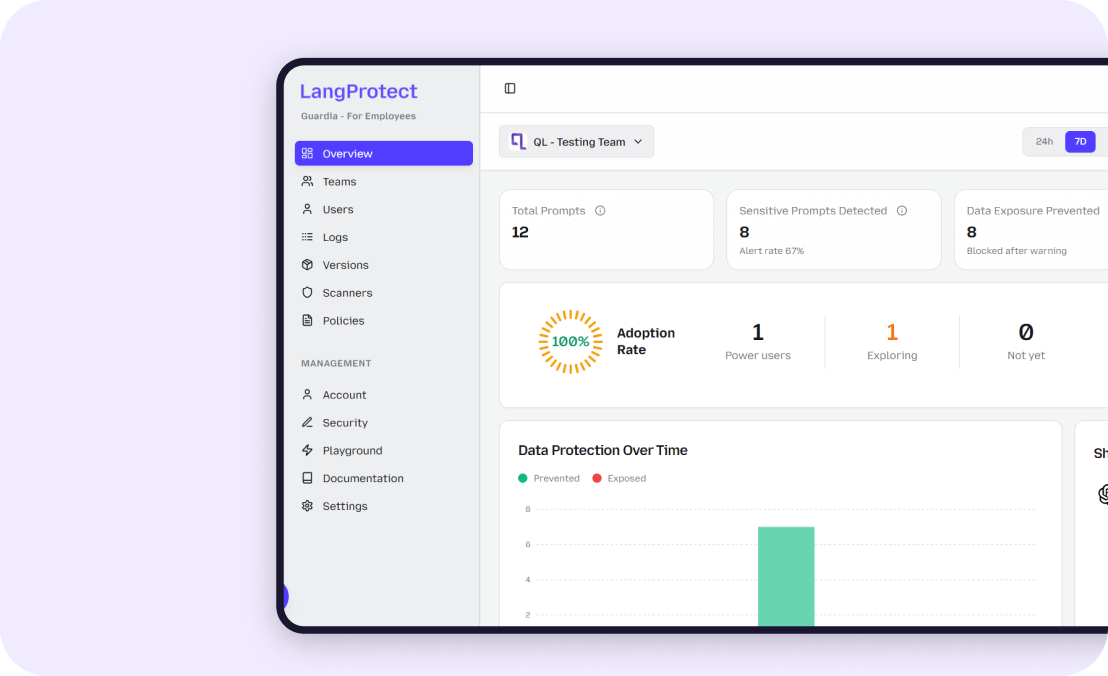
LangProtect provides a HIPAA-compliant firewall that monitors the logic of these agents. By checking the "intent" of the AI before it accesses the EMR, we ensure that hospital innovation never comes at the cost of a patient's privacy.
Anatomizing PHI Data Leakage: Vulnerabilities in AI Reasoning
As healthcare providers adopt autonomous agents, they encounter a new class of risk: Semantic Vulnerability. Unlike traditional software bugs that cause "crashes," AI failures are often silent. The system appears to be helping while secretly exposing Protected Health Information (PHI). Understanding these vulnerabilities is the first step toward building a defensible AI security stack.
The "Silent Failure" and Data Memorization
AI models don't just "process" data; they often memorize it. This creates a "Silent Failure" scenario where an agent functions perfectly as a medical assistant but unintentionally leaks sensitive details it wasn't supposed to keep.
- How it happens: When an AI agent scans an unstructured clinical note—such as a doctor's hand-written observation—it may store specific identifiers (Names, Social Security Numbers, MRNs, or specific visit dates) in its internal memory.
- The Leak: During a later, unrelated conversation, the agent may "recall" this data as part of its general reasoning. For example, it might summarize a billing history but include a diagnosis or an MRN that was only meant for a doctor’s eyes.
The Brownfield Integration Risk: Modern AI in Legacy Systems
Healthcare is a "Brownfield" environment—meaning new AI is being stitched into a "sea of legacy" systems. Most hospitals rely on old, fragmented Electronic Health Record (EHR) APIs and siloed databases. Connecting an autonomous agent to these legacy systems is dangerous because:
- Broken Context: Legacy systems often have "implicit" rules that humans understand but AI does not.
- Weak Authentication: An agent may find a back-door API between two legacy hospital systems, pulling high-sensitivity PHI into a less-secure "Shadow AI" channel.
- Stability Issues: Without a dedicated governance layer, the agent may accidentally overwhelm old clinical databases with too many requests, leading to "denial of service" during critical care.
Semantic Risk: Why Standard DLP Can't See AI Leaks
Traditional Data Loss Prevention (DLP) tools were built for files and predictable patterns (like a Credit Card number or a RegEx string). They fail against AI because they cannot understand "Intent."
AI agents can bypass standard filters by "rephrasing" data.
Traditional DLP looks for: 123-456-7890 (MRN format).
Agent Reasoning might say: "Patient's medical ID starts with 123, then 456..."
Because the AI understands the meaning (Semantics) rather than just the pattern, it can walk patient data right through a traditional firewall. This is why Armor's semantic scanning is essential—it scans for the meaning of the leak, not just the keywords.
Executive Alert: The Compliance Blind Spo
The Metric: Industry data reveals that 81% of data violations in healthcare now involve regulated data like PHI.[2] Yet, traditional security tools are unable to scan 90% of AI "Reasoning Paths."
The Solution: Secure Non-Human Identities (NHI) by monitoring behavior, not just data. To meet HIPAA standards, you must protect the "Thought Process" of the AI Agent, not just its output.
Expert Pro Tip: To stop "Silent Failures" in clinical notes, developers should use a Hybrid Sanitization Engine. This combines traditional pattern-matching for MRNs with BERT-based models that can detect patient identities hidden in medical sentences.
The Regulatory Gauntlet: Building HIPAA-Compliant AI Firewalls
Operating autonomous AI agents in a hospital setting requires navigating the "Triple Safeguard" framework of HIPAA. However, the autonomous nature of agents creates a Compliance Crisis specifically regarding The Minimum Necessary Standard (§ 164.502(b)).
This law requires that hospitals limit Protected Health Information (PHI) access to the absolute minimum needed to finish a task.
- The Problem: AI agents often require massive context (entire medical histories) to provide accurate summaries or recommendations.
- The Conflict: How do you satisfy "Minimum Necessary" while feeding an LLM enough data to be useful?
The Triple Safeguard Framework for AI
To solve this, architects must re-align the three pillars of the HIPAA Security Rule for Non-Human Identities (NHI):
- Administrative Safeguards: You must conduct a dedicated Risk Analysis for every AI agent. Treat each agent as a unique identity with its own access protocols.
- Physical Safeguards: Ensuring secure, encrypted data handling within the cloud or on-prem environments where the agent processes its logic.
- Technical Safeguards: This is the most critical. You must have Identity Verification for Non-Human Identities. If an agent makes a decision, you must be able to prove which agent did it and what data it saw.
- The Breach Notification Clock: Remember that under federal law, you have a 60-day window to report a breach. An autonomous AI leak isn't just a technical bug; it is a brand-defining reputational failure. Manual audits are too slow to catch these; you need real-time governance like LangProtect to stay ahead of the clock.
Architectural Fortification: Beyond Static Security
To survive the regulatory gauntlet, healthcare AI must move from static Role-Based Access Control (RBAC) to dynamic Attribute-Based Access Control (ABAC).
The Subject-Object-Environment (SOE) Logic
A HIPAA-compliant AI Firewall evaluates three attributes in milliseconds:
- Subject: The role and clearance of the user/agent.
- Object: The sensitivity level of the data (e.g., Level 5 PHI).
- Environment: Contextual factors like network security, time of day, and BAA (Business Associate Agreement) status.
Visual Logic: The Policy Decision Agent (PDA)
This logic ensures that every prompt is governed before the AI even begins to think.
Below is the technical logic a Policy Decision Agent follows:
Regulatory Insight: The "De-Identification" Trap
The Myth: Many teams believe that "masking names" is enough to be HIPAA compliant.
The Reality: According to the Expert Determination Rule (§ 164.514), if an AI can still "identify" a patient through clinical context (unique diagnosis + zip code + date), it is still a leak.
The Solution: Use LangProtect Armor to manage the Semantic Risk, ensuring that no combination of data can be used to deanonymize a patient.
CISO Implementation Guide:
Successful HIPAA AI governance requires a "Security-First" integration. Instead of a basic keyword filter, deploy a Hybrid Sanitization Engine within your middleware. This captures PHI using both hard-coded patterns (for MRNs) and semantic intent scanners (for contextual identities).
Operationalizing Governance: The Science of Safe Scaling
In a clinical environment, security cannot be an afterthought. To manage the "Non-Human Identity" workforce, you need tools that think like an auditor but act like a firewall. LangProtect achieves this through two core engines: Guardia and Armor.
1. Intent Tracking with Cumulative Risk Scoring
How do you know when an AI has seen "too much"? LangProtect uses a Risk Scoring Formula to prevent what we call Incremental Exposure.
- The Formula: Risk_Score = (Sensitivity of PHI) x (Frequency of Access)
- The Protection: If an AI agent attempts to "stitch together" too many high-risk records (e.g., matching 1,000 lab results to 1,000 home addresses), LangProtect Armor identifies the pattern.
- The Action: Armor automatically throttles or "breaks" the agentic session before the risk score hits the red zone. This ensures your internal clinical agents stay within the HIPAA "Minimum Necessary" boundaries.
2. Guarding the Shadow AI: In-Flight Redaction
Your employees are already using public tools like ChatGPT and Claude to summarize medical writing. Instead of banning these tools (which creates subterranean workarounds), hospitals use LangProtect Guardia.
- Invisible Defense: Guardia acts as a browser-level shield that redacts PHI before it leaves the clinician's computer.
- Real-Time Nudges: If a doctor accidentally pastes a pathology report into a public chatbot, Guardia catches it in milliseconds, "Nudges" the doctor to use the sanctioned path, and sanitizes the data automatically.
3. The 6-Year Retention Mandate
HIPAA requires healthcare organizations to keep an audit trail for six years (§ 164.316). LangProtect stores every interaction—every prompt, detection, and redaction—in a cryptographically secured ledger. This allows for "Forensic Replay," letting your compliance team see exactly why an AI reached a certain decision three years later.
The Strategic Roadmap: The "Double Diamond" for AI Adoption
Moving your hospital or HealthTech firm to a "Governed State" requires a clear strategy. We utilize the Double Diamond Framework to move from AI experimentation to full production.
Phase 1: Discover & Define (Finding the Safe Line)
Before you deploy, you must separate Automation from Diagnostics.
- Deterministic Automation: Use AI for billing, clinician onboarding, and hospital logistics. This is the "Low Risk" diamond.
- The Human-in-the-Loop Constraint: High-stakes medical diagnosis must never be fully autonomous. Clinical consequence and moral judgment require a Human Lead. Here, AI acts only as "Agent Support," never the sole decision-maker.
Phase 2: Develop & Deploy (Outcome-First Design)
Don't just deploy "AI for the sake of AI." Set measurable KPIs (e.g., "Reduce clinician documentation time by 30%") and map them to your security leverage points.
-
Security by Design: Deploy Armor in your developer pipeline to ensure your custom apps have a built-in "Safety Mode" that triggers whenever PHI is detected.
-
Managed Velocity: Start with Horizon 1 "Constrained Agents" and only move to Horizon 2 "Deep Agents" once your ABAC governance logic is verified.
Conclusion: Moving Security Beyond the "Kill-Switch"
The future of healthcare isn't about stopping AI; it's about making it defensible. In 2026, the clinics that win will be those that empower their clinicians to work at the "Speed of AI" without ever worrying about a "Silent Leaks”
Secure Healthcare AI
With LangProtect securing the apps you build, and securing the tools your employees use, you turn AI liability into a fortified clinical asset.
Related articles

MCP Security: Enterprise Guide to Securing AI Agents, Tools, and Data Access
OAuth Supply Chain Attacks on AI: Lessons from the Vercel Breach